There are many natural variations in anatomy that can be found in the thoracic outlet, including:
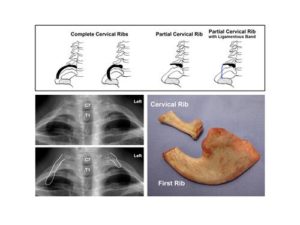
- Cervical (extra) rib – complete or partial
- Bony anomalies of the first rib
- Variations in soft tissues, such as muscles and ligaments
The most obvious of these variations is a congenital cervical rib, an extra rib that occurs in approximately 0.5% of the population. Cervical ribs, both complete and partial, can usually be detected by plain X-rays of the chest or neck.
In some individuals, there is an even shorter segment of extra bone that is simply considered to be an unusually wide C7 transverse process; although this is not considered an extra rib, a wide C7 transverse process can be associated with a ligamentous band just like a partial cervical rib. Other rare bony anomalies can affect the first rib alone. Any of these anomalies may predispose to the development of TOS.
Variations in the soft tissues of the thoracic outlet have also been described. These variations are often too small to be detected by standard imaging tests, such as plain X-rays, CT or MRI scanning, but they are frequently seen at the time of surgery. When present, any of these structural variations in soft tissue anatomy can contribute to nerve or blood vessel compression.
Examples of soft tissue variations include:
- Scalene minimus muscle – a variant in which a small muscle passes between the nerve roots of the brachial plexus, and then attaches to the first rib along with the anterior scalene muscle
- Ligamentous or fibrofascial tissue bands – described as a fibrous band that runs from the back of the first rib to the front, crossing over (and compressing) the lower nerve roots
- Accessory phrenic nerve – a small extra branch of the phrenic nerve passes in front of the subclavian vein before turning down into the chest